
Welcome back to Squat University! Today I want to introduce a simple guide to help you figure out which type of knee pain you may have.
When most people develop knee pain while barbell training, they’ll receive a vague diagnosis from the doctor of “Patellofemoral Pain Syndrome” (PFPS). Unfortunately, this is a junk term that covers several possibilities. Some have described it as a ‘condition of many conditions’ as the name is often overused as an acceptable diagnosis without a clear understanding for the source of pain. Using such an ambiguous term only leads to confusion.
In 1998 four leaders in the field of sports medicine and rehabilitation (Kevin Wilk, George Davies, Bob Mangine, and Terry Malone) came together to develop the most detailed classification for patellofemoral syndrome or generalized knee pain.2
By separating the different causes of knee pain into special categories, it allows for a better understanding for how to fix the problem.
Listed below are common knee injuries that barbell athletes sustain.
- Iliotibial Band Syndrome
- Patellofemoral Compression Syndrome
- Biomechanical Dysfunction (aka Bad Technique)
- Patellar and Quad Tendinopathy
There are other causes of knee pain, of course, but a large majority of the problems I see with barbell athletes can be traced back to these four diagnoses.
ILIOTIBIAL BAND SYNDROME
The IT band is a thick band of fascia that starts at the hips and runs the entire length of your leg, connecting to the outside part of the patella (knee cap), tibia, and lateral hamstrings (biceps femoris tendon).1 This pain usually presents on the lateral part of the knee and is caused by excessive compression of the band as it pushes into the fat pad that covers the prominent bony part of the femur (lateral epidondyle). Symptoms often grow over time and aren’t often linked to one specific incident or trauma (like getting hit on the side of the leg).

The location of pain is actually one of the best diagnostic tools for differentiating IT Band Syndrome from other forms of knee pain. While this pain can start off dull and achy, it can often progress to a sharp pain that you can pin point to one specific area on the lateral surface of the knee where the band inserts. Some people will even complain of a painful “popping” or “snapping” sensation at times.
This injury will not create pain often around the knee cap, as that symptom is usually reserved for the next two diagnoses (compression syndrome and biomechanical dysfunction).
PATELLOFEMORAL COMPRESSION SYNDROME and BIOMECHANICAL DYSFUNCTION (LATERAL PATELLA TRACKING)
If you have pain generally around your knee cap (patella) or directly underneath it, you’re likely dealing with one of two issues: a tracking/compression issue of the patella or a biomechanical dysfunction. This pain usually increases in intensity the more you lift (squatting 100 lbs. may bring out 1/10 pain while 300 lbs. will create 5/10 intensity).
As you move your knee, your kneecap travels within a small notch in your femur called the patellar groove. As your knee bends and straightens the tissues (muscles and fascia) that surround the joint keeps the patella traveling in a stable position. If, the patella fails to track and move correctly within this groove, injury can occur.
For example, when the tissues that surround the knees are stiff and bogged down, the patella will be smashed into the femur’s groove. This type of compression can cause the patella to shift and tilt to the side (creating uneven pressure on the underside of the bone). When this occurs, it can create pain under the kneecap where there is excessive pressure between the two bones (femur and patella) or on the inner or medial side where the tissues are being stretched out.
Poor knee control (instability) can also cause the patella to sit and track incorrectly within the femur’s groove. Poor technique when barbell training can lead to knee pain (this is the most common reason why!). Even the most subtle problems in knee control can lead to the gradual development of pain over time.

When I screen an athlete who has knee pain, I ask them to first perform a bodyweight squat without shoes on and with their toes straight relatively forward (about 5-7 degrees of toe out angle). In order to perform a good full depth squat the athlete must have good ankle and hip mobility, adequate core/pelvic control, sufficient balance and knee control.
Next I will ask the athlete to perform a single leg squat on each side. You have to be very observant during this part of the examination (taking video of this movement can be helpful for review) as even the smallest differences in side to side mechanics may be the reason behind the current symptoms. Many athletes will be strong enough to “hide” their imbalances in mobility or stability when on two legs. However, when you challenge them to squat with one leg then the once “invisible” problems are now uncovered.

The “why” behind both compression and tracking injuries of the knee can often be traced back to a deficit or “weak link” in either mobility and/or stability. For example, did you notice what happened at your own feet during the single leg squat?
The foot is like your body’s house of cards’. Its stability sets the foundation for the rest of your body to move. When the foot collapses over (pronation) it leads to rotation in the tibia that forces the patella to move laterally.3 This same problem (wobbly knees) can also occur due to poor hip coordination that leads to knee collapse during the squatting motion. If you only poked and prodded around the knee during your examination and never take a step back and take into account the entire person in front of you, you’ll miss valuable insight into why your injury occurred.

Flexibility and mobility issues in the lower body can also create a number of movement problems that lead to knee pain. For example, limited ankle mobility or stiffness in the lateral hamstrings can lead to excessive toe-out angle during the squat that again pulls the patella laterally. When the knee moves in this off-axis manner with enough repetition, pain eventually develops around the kneecap. We will go over how to screen for this later on.
PATELLA AND QUAD TENDINOPATHY
Athletes who are involved in sports that include sudden explosive and repetitive movements of the knee can develop pain and tenderness at these tendons. Of the two, patellar tendon pain is usually the more common injury especially in sports such as basketball and volleyball due to the excessive jumping (this is where the term “jumper’s knee” was coined). Interestingly enough, it is due to the high volume of jumping rather than the amount of running that facilitates these injuries as running usually doesn’t place high enough load on the tendon to create symptoms.5 Patellar and quadriceps tendon pain are also prevalent in sports such as weightlifting, powerlifting and CrossFit due to the high forces that are sustained during the repetitive strength and ballistic movements.

Classically, those with patellar tendinopathy will complain of tenderness and pain at the connection point of the kneecap and patellar tendon (called the inferior pole of the patella).6 You may even experience pain where the patellar tendon attaches to the tibia (a small bump on the front of your shin called your tibial tuberosity). Usually you won’t have pain directly in the center of your patellar tendon unless you’ve sustained a direct blow to the knee (like hitting your knee into a corner of a desk). Those with quadriceps tendinopathy will have pain and tenderness at the connection point of the kneecap and the quad tendon (called the superior pole of the patella).
Do not assume that you have patellar or quad tendinopathy just because of the location of your pain! Poking and prodding tender tissues is not enough. This is one of the most common pitfalls to the diagnostic process and can lead you down the wrong path of treatment!
Also, do not rely on medical imaging to diagnose yourself with tendinopathy! Many times people will have imaging that shows degrading pathology in the tendons, however the source of their knee pain is actually something!4
There are two hallmark features of tendinopathy:4,5
- Pain remains localized to the inferior pole of the patella (you should be able to point directly to where your pain is and it should not move as you perform different activities).
- The intensity of your pain is proportional to the amount of energy stored in your tendon. The more you use your tendon like a spring, the more pain you have (a reason riding a bike will never create tendinopathy as the tendon is not used in that manner).
With these key points in mind, try these simple tests. Perform your basic bodyweight squat again and rate your pain from 0-10 (zero being no pain and ten being the absolute worst pain you could imagine). Next, perform 10 tuck jumps in a row as high off the ground as you can without any rest in between each jump. Did your pain intensity go up? If it did increase, did the pain remain localized to the inferior pole of the kneecap or did it start to spread over time to other parts of the knee joint? Compression and tracking issues rarely co-exist with patellar tendinopathy so make sure you can clearly answer each of the prior questions.
DIAGNOSING YOUR KNEE PAIN
| IT Band Syndrome | Patellofemoral Compression Syndrome or Biomechanical Dysfunction | Patellar & Quad Tendinopathy |
| Pain is on the side of the knee just above the bony prominence (lateral epicondyle). Your kneecap is not sensitive to touch. | Pain is located in or around the kneecap. It is not comfortable to push on your kneecap while contracting your quads. | Pain can be localized to either above or below the knee cap (often in the tendon that attaches to the bone). It will remain localized and increase in intensity as you increase load and use the tendon as a spring.
|
OTHER HELPFUL TESTS
5 inch Ankle Mobility Screen
Testing ankle mobility should always be a part of the screening process when dealing with a knee injury. For example, if the gastroc and/or soleus muscles are stiff or short, there is less range of motion to absorb load during activities like landing from a jump. For example, research shows that between 37-50% of the total forces absorbed by your body when landing from a jump occur at the ankle joint.8 Ankle stiffness therefore reduces the capacity of the body to absorb energy in this manner, which means higher loads are transferred up the body to the patellar tendon. Therefore, the patellar tendon is placed under greater strain as the tendon has to take more loads more quickly, increasing the risk of tendinopathy.9
Limited ankle mobility can also play a part in changing how our knee moves when we perform movements like a squat, clean or jump. In the book Anatomy for Runners physical therapist Jay Dicharry, uses a perfect metaphor for describing how these types of restrictions change our movement patterns.10 If you have ever driven your car through a European-inspired roundabout, you know that you can’t just drive straight through the intersection. You have to go around the center island.
An ankle with full mobility will allow the tibia to move freely on the foot. Think of this like a car being able to move straight through an intersection. A bony block is like a roundabout in the intersection. When the car enters the intersection, it must now go around the island in order to proceed on its previous route. Essentially our lower leg spins off its normal route and falls inward. As our lower leg goes around the bony block, the knee is pulled inwards. Movement breaks down. Limited ankle mobility is therefore a potential factor in why someone could develop a patellar tracking or compression injury!
The 5 inch wall test is a very simple screen you can perform on your own.11,12 Kneel down by a wall and place your toes five inches from its base. Drive your knee straight forward over your toes attempting to touch the wall without letting your heel pop off the ground.


What did you find? Were you able to touch the wall with your knee, or did your heel pull off the ground? If you failed the 5-inch wall test, you just uncovered a weak link in ankle mobility that needs to be addressed.
SINGLE LEG BRIDGE SCREEN
It is common to see strength deficits and coordination issues in how muscles are activated at the hip with athletes dealing with knee pain. In my experience, many athletes demonstrate underactive or weak glutes. A simple screen to expose this weakness is a single leg bridge test.
Lay on your back with one leg bent and the other straight. Perform a single leg bridge and hold the highest position for 10 seconds. What muscles did you feel working hard after holding this single-leg bridge for 10 seconds?
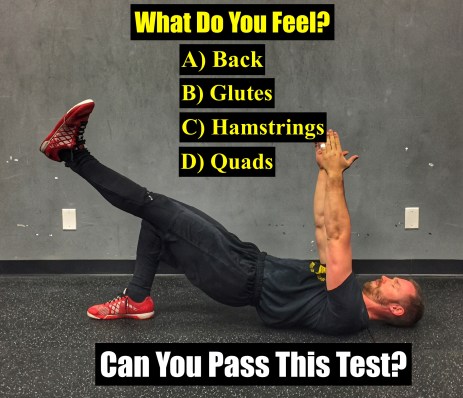
Our goal with this screen is to identify your “go-to” muscles for hip extension (the movement that drives you out of the bottom of the squat, clean, snatch, etc.). If you felt anything other than your butt muscles (glutes) working hard, you have a coordination and/or strength problem we need to work on.
TAKE AWAY
Finding the source for you aching knees can be a daunting task, however with the proper diagnosis we’ll be able to better direct you in fixing your pain. None of these injuries will bring out locking or clicking of the knee, significant swelling, tingling, numbness, or throbbing in the back of the knee. If you have any of these symptoms, it’s likely an indication of a more significant problem that requires a medical evaluation by a professional.
Until next time,

With

References
- Khaund R & Flynn SH. Iliotibial band syndrome: a common source of knee pain. American Family Physician. April 15, 2005; 71(8): 1545-155
- Wilk KE, Davies GJ, Mangine RE, Malone TR. Patellofemoral disorders: a classification system and clinical guidelines for nonoperative rehabilitation. JOSPT. November 1998; 28(5): 307-322
- Sammarco GJ, Burnstein AH, Frankel VH. Biomechanics of the ankle: a kinematic study. Orthop Clin North Am. 1973; 4(1):75-96
- Rio E. Isometrics for tendon pain. Practical implementation and considerations. Sports Health. 2016;34:33-35
- Cook J, Rio E, Docking S. Patellar tendinopathy and its diagnosis. Sports Health. 2014;32(1):17-20
- Rudavsky A, Cook J. Physiotherapy management of patellar tendinopathy (jumper’s knee). Journal of Physiotherapy. 2014;60:122-129
- Malliaras P, Cook JL, Kent P. Reduced ankle dorsiflexion range may increase the risk of patellar tendon injury among volleyball players. J Sci Med Sport. 2006;9(4):304-9
- Devita P, Skelly WA. Effect of landing stiffness on joint kinetics and energetics in the lower extremity. Med Sci Sports Exerc. 1992;24(1):108-115.
- Backman LJ, Danielson P. Low range of ankle dorsiflexion predisposes for patellar tendinopathy in junior elite basketball players: a 1-year prospective study. Am J Sports Med. 2011;39(12):2626-33
- Dicharry, J. (2012).Anatomy for Runners. New York, NY. Skyhorse Publishing.
- Bennell K, Talbot R, Wajswelner H, Techovanich W, Kelly D. Intra-rater and inter-rater reliability of a weight-bearing lunge measure of ankle dorsiflexion. Australian Journal of Physiotherapy. 1998; 44(3):175-180.
- Reinold M. (2013) Ankle mobility exercises to improve dorsiflexion. Retrieved from MikeReinold.com.
I have a constant knee click on both knees, they dint particularly hurt but will feel achey after squatting heavy. Any recommendations on what to do to correct this issue?
Thank you for the article.
What can cause knee pain on inside side of the leg?
Best,
Natalia
Nice article.
I would be very interested in reading about possibilities to fix Patella Tendonitis.
Hello Dr. Horschig,
In no regard am I comparing qualifications in relativity better the education required between being a doctor in physical therapy and a certification. In that regard, I have a degree in Kin and I am now considering a “Corrective Exercise Specialization”certification through the National Academy of Sports Medicine, which focuses on injury prevention, movement analysis, etc, along with maybe obtaining a degree as a Physical Therapy Assistant. Any thoughts on these ? I know you are extremely busy!
Put me on your email list
Very nice info. I love it thank you for sharing Dr.
Do you have these posts already? I have knee pain for months now, I could handle it but stops me to improve in any weightlifting aspects 🙁
[…] back to Squat University! For the past 2 weeks we’ve been discussing common causes of knee pain when barbell training. In this article we’re going to dive a little deeper into IT Band Pain […]
I do consider all of the ideas you have offered
on your post. They’re very convincing and can certainly work.
Still, the posts are too brief for newbies. May just you please prolong them a bit from subsequent time?
Thank you for the post.
Will do! Thanks for the suggestion!
[…] back to Squat University! For the past few weeks we’ve been covering the topic of knee pain. Today I want switch gears and introduce a new series on hip […]
Love your articles so helpful…. i have more than one, it has been ease out but is any diagnosis when the pain is at the head of the fibula and peroneal????…. thanks again…
There can be a few things that can lead to pain in that area. I’d personally recommend going to see a physical therapist for a hands on evaluation to truly find what’s going on and the most efficient way to fix it.
[…] What Kind of Knee Pain Do You Have? […]
Love you articles, very informative and helpful.
I have had IT band release surgery on my right knee after 7 years of pain and on/off physio. All in all the surgery seems to have relieved the ITB symptoms.
I recently started to get the ITB symptoms in my left knee. Do you have any information or details how to help treat this? I don’t want another 6 months off training recovering from more surgery so would like to sort it sooner rather than later.
Many Thanks
My knee pai go3s from knee #own one side of leg & to my ankle. I was diagnoses with swollen nerve, yesterday leaned over & felt a stretch on the back of my knee. The pain was EXTREME. IN what category do i fall in
Thank you Do”tor.
I am 80 years old.
How do I fix a knee that doesn’t leave 155-degree angle without popping or cracking
In patellar grinding test, Why u were checking in different knee angle like 30 and 60 degree?
[…] knee, chances are you don’t have a tendinopathy injury. You have a higher likelihood of having patellofemoral pain in this […]
Good morning Dr. Horschig,first of all thank you for your work and sharing, I find it really useful and precise.
Just a quick question: what if I have all the problems you listed? IT Band Syndrome, Patellofemoral Compression Syndrome and Biomechanical Dysfunction (patella moves outwards) and patellar & Quad Tendinopath? I had two surgical (complete elimination of meniscus + reconstruction of acl 20 yrs ago, yet a lot of issues with knee like hard grasping,bad tendon pain, IT band pain etc.).
Thank you very much.
Dear Aaron,
I follow you in social network for a long time.
This article is very interesting but it doesn’t screen my concern.
My knee doesn’t hurt, it is just like if it wanted to “come out” or “separate” when I get up from a chair or I walk up the stairs. A strange sensation happens in the outside part of my knee, in the “hole” to the right of the patellar tendon.
I can squat, run, jump… But with some particular moves my knee feels weak and like if it wanted to slip away.
Do you happen to have any idea of what I mean?
Thank you in advance.
Best regards, Javier
Hello I’ve been having pain in the bottom left part of my quad near the knee cap and also a lot of soreness on my tibial tuberosity area for days after squats what could be the underlining issue
I have knee pain in both knees. Knees are sensitive to direct contact with the ground ( When I get on my keens). I have full range of motion but very slow moving getting off the ground.
I never leave comments but this article about knee pain was such a great help, found the answers I needed.
Thank you very much and keep up with the good work!!
[…] the past few weeks we’ve been discussing knee pain. We started with an article on IT Band syndrome and followed it with another on patellar tendon […]
[…] Knee pain – specifically patella femoral pain syndrome (PFPS), patellar tendonitis and ITB syndrome. […]
[…] squatting, your knee is above a 2 on your (subjective) 1 to 10 scale, take the weight off the bar, reevaluate and fix up your form. If your pain sticks around, see a doctor or PT who specializes in […]
Hey, thanks for taking great initiative of writing a blog on Knee pain as I understand that the pain may vary and if not taken care of could lead to much worse case. The blog is informative and interesting.
[…] If knee discomfort develops, knee sleeves will not necessarily resolve the issue. It is best to consult a physician with an understanding of weightlifting in order to determine if an issue with lifting form is causing knee discomfort. A good place to start would be this article on knee pain by Squat University. […]
[…] Source: 🔗 […]
[…] Source: 🔗 […]
Squat University often publishes useful information for those who want to learn the basics of proper training and medicine. When I was researching nurse essays https://gradesfixer.com/free-essay-examples/nurse/ I found some of your stuff. At the university, I was actively involved in sports, but unfortunately, due to an injury, I can no longer continue my sports career. But I discovered a new passion for myself. I want to be a nurse and help in the sports rehabilitation department. Knee pain is one of the most common problems in modern rehabilitation and I am very grateful to you for your educational materials.
The article provides diagnostic criteria for each type of knee pain and suggests some simple tests to help individuals identify which type of knee immaculate grid pain they might be experiencing. It also highlights the importance of addressing underlying factors like ankle mobility and hip muscle activation in managing and preventing knee pain.
I would like to introduce a new game – Getaway Shootout is a great game for anyone who wants a quick, fun, and challenging game. It’s perfect for casual gamers and hardcore gamers alike.
Hi Doctor. When I squat I do not have pain in my knees, however after squatting I have a burning sensation in both of my knees. When I do lunges the pain in my knee cap is around 2 out of 10. This pain started 4 weeks after I resume martial arts training. Looking for some advice on how to determine if this is Patellofemoral Compression Syndrome