Do you have groin pain that feels like a pinch in the front of your hips as you move into a deep squat? This symptom is one of the most common complaints of those who have a hip impingement (called femoroacetabular impingement or FAI).

If you think you have this injury, make sure to check out THIS ARTICLE and perform the three tests I describe. If you only had one positive test out of these three, the chances of having a hip impingement is fairly low. 1,2 However, if you tested positive for all three tests (C-Sign, log roll and FADIR test), the likelihood of having this injury is high and you may benefit from the following corrective exercises listed today.
Finding The Cause
Hip impingement usually presents in young-adult athletes (early 20s to mid-30s), who experience a slow onset of groin pain due to a repetitive pinching between the femur and the front of the hip socket (acetabular rim). This contact between the two bones usually occurs in movements that require a ton of hip flexion (such as sitting into a deep squat).
As you squat, the femur rotates inside the hip joint. For those with normal “textbook” anatomy, the femur always maintains a little space (about 9mm) from the front rim of the hip socket.5

There is often a degree anatomical variation from person to person. Simply put, not everyone has a “textbook” bone structure (especially when it comes to the hips). Changes in the way our bones align can lead to a “blockage” of movement when you try to get into certain positions (like a deep squat or lunge).

For example, if we look at the pelvis we find that some people have hip sockets that open more to the side and others that open at a more forward angle. A hip socket that opens laterally (called acetabular retroversion) creates more coverage around the front of the femur (which can lead to an impingement between the two bones in a deep squat).

The shape and alignment of the femur as it connects to the pelvis can also lead to an impingment.3 For most of us, our femurs normally align with the pelvis at a slight forward angle. However, some of us have femurs that are twisted slightly forwards or backwards. A more forward angled femur is called an anteverted femur. A more flattened angle is called a retroverted femur.4 Research has shown that a retroverted femur can often increase pressure at the front of the hip joint with certain movements and cause impingement.6

Getting to Know Your Anatomy
We can start our screening process by simply observing how someone stands. Stand in a comfortable stance with your feet around shoulder width. Look for the position of the feet and which way the toes are pointing.
A “duck stance” or exaggerated toes out stance is often seen with those with retroversion. This position feels normal because the backward twist of their femur leaves them with the appearance of having excessive external hip rotation. This position however isn’t due to limited flexibility but rather because their bones are shaped in a way that sets a new “normal” for their movement capabilities.
We however can’t stop our evaluation at this point and definitively say someone has retroversion just because they stand like this. Turning the toes out excessively can most certainly be a sign of poor hip mobility (something we can modify). There will also be those with hip impingements who will not show a toed out foot position in their normal stance. For this reason, we need to perform some testing to find what is truly at fault.
A test you can easily perform at home to check for femoral retroversion is called Craig’s test. Start by lying on your stomach with your knees bent at 90°. Have a friend take their hand and feel for the where the notch of the femur (greater trochanter) is located on the side of your hip. With their other hand, begin rotating your lower leg in and out. As the leg rotates, the tester will begin to notice the notch of the femur becoming more and less prominent against their hand. Stop moving the lower leg when they find this position to be most prominent.
‘Normal’ anatomy will leave the lower leg pointing slightly away from the body (within 15° from a vertical position). If the athlete has their lower leg now positioned directly vertical or angled slightly in towards the rest of the body, they have a retroverted femur. This method of assessing hip anatomy has been shown in research to be extremely reliable (even better than taking an X-ray).8,9
We can now perform a test to give us a better understanding of the position of your hip socket. Start by lying on your back. Have a friend bring your knee towards your chest in a straight line. See how far your thigh can move before feeling a “blocked” sensation. Next, perform the same movement but allow the thigh to move out to the side and the foot to rotate inwards slightly (an abducted and externally rotated position of the hip).
Were you able to now move the knee further towards the chest without a pinching or blocked sensation? Research as shown that those with retroverted hip sockets will often be able to bring their knee closer to their chest with the knee out to the side.10
Can We Fix It?
If you have a hip impingement and found it to be related to your anatomy, there are two non-surgical options to decrease your pain:
- Change your stance
- Try to Improve hip capsule mobility
Stance Considerations
While most people should be capable of performing a bodyweight squat with their toes relatively straight forward (5-7° toe out angle) that does NOT apply to everyone. If you suspect your body has femoral or acetabular retroversion, it is going to be “normal” for your body to have a more exaggerated toe out angle (>30°) when you squat, catch a clean/snatch or dead lift.

If you found a possible retroverted hip socket or femur in the previous tests, try this squat test. Assume a bodyweight squat stance with your toes relatively straight forward. Try to squat as deep as possible. Next, point your toes out to approximately 30° and perform the same deep squat. Patients with retroverted hips will often feel an uncomfortable and painful sensation in the front of their hips that limits depth during the squat with toes forward.7

What this means is your body has a bone structure that does not allow for a straightforward foot squat. It is normal and natural for your body to squat with your toes angled out and no amount of mobility work will significantly change this.
Banded Joint Mobilizations
While we can’t change your bony anatomy, we can hope to improve the mobility of the tissues that surround the hip joint (hip capsule). Most researchers believe that those with hip impingements may also have restrictions in the lateral and posterior portions of the hip capsule fibers.

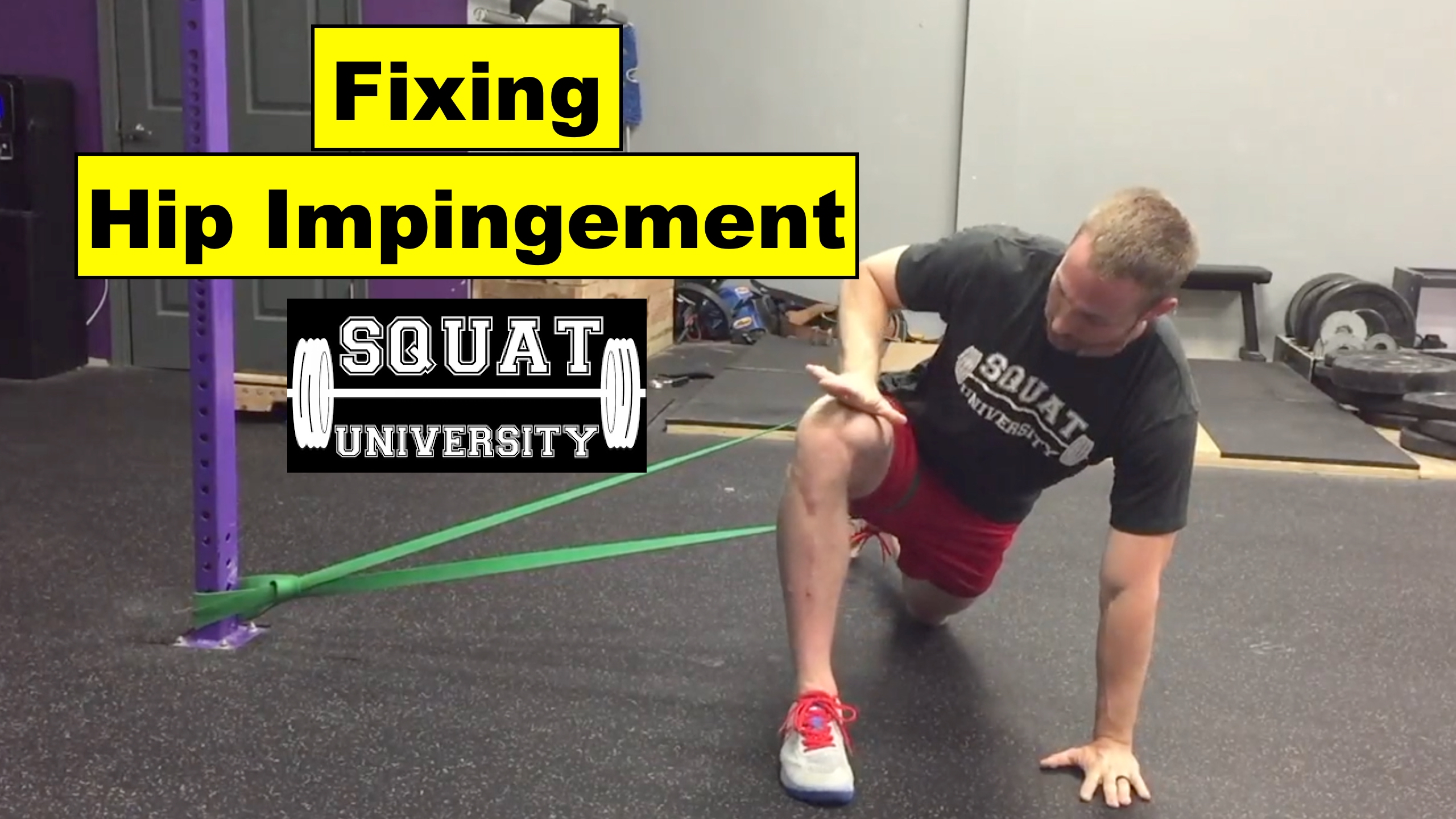
The first exercise I want to show you is the lateral banded joint mobilization.11 Place a long resistance band around your thigh (try to get it as high as you can towards your hip). Get a ton of pressure on the band as you assume a kneeling lunge, with the hip you want to work on in the forward position.
Once in the lunge, take your hand and pull your forward knee across your body and back to the start position. This movement (along with the pull from the band) will help stretch the lateral and posterior fibers that surround the hip. If the band is pulling hard enough, the inward knee movement should not bring out any pinch-like pain in the front of the hip but instead a possible light stretch to the side of the hip.
Next, with the band still around your thigh, take your forward knee and place it into the ground. Your thigh should be positioned around 90°. From this position pull your torso toward the ground and rock your hip to the side (towards the pull of the band). This posterior-lateral motion will bring out a stretch to the back and side of your hip. Hold this motion for ~10 seconds before returning back.
In this position you can also externally rotate your hip by moving your foot towards your stomach. This may increase the stretch feeling to the lateral hip.
Recommended sets/reps: 2 minutes of slow rocking movements
Pigeon Stretch
We can also stretch the posterior hip capsule without a banded joint mobilization with a stretch called the pigeon stretch. Find a high bench or bed and place your leg on top in an externally rotated position.
With your lower leg completely flat on the bed, lean your torso forward until you feel a light stretch in your hip. Make sure to keep your back from rounding during this movement. You can play around with this movement and lean your torso in different angles (towards your foot or your knee for example) to maximize the stretch in the back of your hips.
You can also perform this stretch on the ground if you don’t have access to a table.
Recommended sets/reps: 3 sets of 30-second stretch
Final Thoughts
Not everyone has ‘textbook’ bone structure and trying to conform to a squat stance that isn’t right for your body can be disastrous. If you have a hard blocking sensation or a pinching pain in your hips when lifting, this is your body telling you to move differently. Listen to it.
Just because you didn’t hit the genetic lottery with getting perfect hip anatomy doesn’t mean you should hang up your weightlifting shoes and quit training altogether. You only need to understand what technique adjustments and the necessary mobility modifications your body requires in order to reach your potential and stay pain free. If your pain continues to persist or worsen despite trying these interventions, I highly recommend seeking out a medical doctor to see if there is any serious issues that may need surgical intervention.
Until next time,

with

References
- Laborie LB, Lehmann TG, Engesaeter IO, et al. Is a positive femoroacetabular impingement test a common finding in healthy young adults? Clin Orthop Relat Res. 2013 Jul; 471(7):2267-2277
- Tijssen M, van Cingel R, Willemsen L, et al. Diagnostics of femoroacetabular impingement and labral pathology of the hip: a systematic review of the accuracy and validity of physical tests. Arthroscopy. 2012 Jun;28(6):860-71
- Espinosa N, Rothenfluh DA, Beck M, Ganz R, et al. Treatment of femoro-acetabular impingement: preliminary results of labral refixation. J Bone Joint Surg Am. 2006;88:925-936
- Cibulka MT. Determination and significance of femoral neck anteversion. Physical Therapy. 2004; 84(6):550-558.
- Hossain M, Andrew JG. Current management of femoroacetabular impingement. Curr Orthop. 2008;22:300–310
- Satpathy J, Kannan A, Owen JR, et al. Hip contact stress and femoral neck retroversion: a biomechanical study to evaluate implication of femoracetabular impingement. Journal of Hip Preservation Surgery. 2015;2:287-294
- Sahrman S. Diagnosis and treatment of movement impairment syndromes. Mosby Verlag. 2002
- Ruwe PA, Gage JR, Ozonoff MB & DeLuca PA. Clinical determination of femoral anteversion. A comparision with established techniques. J Bone Joint Surg Am. 1992 Jul;74(6):820-30.
- Souza RB & Powers CM. Concurrent criterion-related validity and reliability of a clinical test to measure femoral anteversion. Journal of Orthopaedic & Sports Physical Therapy. 2009;39:586-592
- Reynolds D, Lucas J, Klaue K. Retroversion of the acetabulum a cause of hip pain. Journal of Bone & Joint Surgery, British Volume. 1999;81:281-288
- Reiman MP & Matheson JW. Restricted hip mobility: clinical suggestions for self-mobilization and muscle re-education. ISJPT. 2013 Oct; 8(5):729-740
**All bone images were used with permission from Paul Grilley
Awesome article, doctor! I wish I had read this three years ago when I reached my peak at powerlifting. Unfortunately, I’ve destroyed my hip joints and have constant stabbing pain every minute of every day… At 26 years old. I’m glad more information is coming out regarding abnormalities in hip anatomy, because I was instructed by several “coaches” to squat with my feet pointing forward. Now I realize I was forcing my hips into an unnatural range of motion and impinging myself.
Michael! Thanks for checking out the article and commenting with your story. I’d be happy to help you as much as I can with your hip issues. If you like, feel free to email me (link on the home page of this website) and we can talk more!
Hi Dr. Aaron! Thank you for this post, it’s very helpful!
I’ve been working hard on improving my hip mobility since July since I’ve been in pain for many years from hip impingement. (not a weightlifter though)
I find the pigeon pose very painful and hard to keep the stretch for more than a few seconds. Sometimes I feel like I’m not improving at all. Do you think that this is expected and what would you recommend for the pain reduction?
Thanks Doc, very useful (and thanks for citing sources too, much more trustworthy). Do you think people with this condition can squat feet outwards and still become successful weightlifters?
You’re very welcome Dom – I’m glad you’re enjoying the content! I would say it is possible, if you watch a lot of olympic weightlifting there are a number of lifters who use a toe out position on the catch of their lifts.
[…] Hip Impingement: See This Blog […]
Thanks for this. Do you have any experience with people squatting post surgery? I have tried mobilisation/stretching/etc/PT for 2 years now and am considering surgical intervention. I’m not sure what to expect if I go for it – will I ever be able to squat below paralell again?
Dr. Horschig, thank you for this video series on banded hip mobilization. It is really nice to see great information like this. Your hip videos are some of the rare ones that will not actually create more impingement. I have just forwarded this to one of my patients.
Great article. How often do you do the stretches? 3 times a day? Every day?
[…] *https://squatuniversity.com/2017/10/21/fixing-hip-impingement/ […]
[…] *https://squatuniversity.com/2017/10/21/fixing-hip-impingement/ […]
[…] *https://squatuniversity.com/2017/10/21/fixing-hip-impingement/ […]
I have had hip impingment for 3 years and am 23. I have tried to keep squatting and deadlifting up until a month ago my good hip had a loud pop and a pinching feeling. I am doing the FAI fix by upright health and GOTROM and am not having much relief. I also went to a local physical therapist and got a routine from him. I have not been able to find out what causes the flare ups because since I stopped squatting and deadlifting a month ago I am in worse pain now. I have a lot of popping clicking and obvious imbalance. I am not willing to get surgery because it is obviously not very advanced as I would have to find the best surgeon in america to have any hope of having a decent result.I appreciate these articles very much.
Thank you, doctor, for the videos. Having recently been diagnosed with FAI with femoral retroversion, I’m hoping some of these exercises will help. My pain is far from debilitating, but I’m somewhat scared of continuing to squat and causing myself more damage – I don’t need surgery yet and would like to keep it that way.
I was previously a very deep squatter and wonder if adopting a wider, toes-out stance and shallower squat depth will be safe enough to continue performing squats? Or should I just abandon the squat entirely and adopt some new exercises instead Does anyone have any thoughts on continuing to squat with this condition?
[…] https://squatuniversity.com/2017/10/21/fixing-hip-impingement/ […]
Thank you for saving me from this excruciating hip pain. Didn’t know where it came from. Everything I tried didn’t work…I saw your video, ordered a band and voila!!!! No more pinching ! I’m not even a power lifter, I’m a runner! Thank you!
Good afternoon Dr. Aaron, how are you?
I would like to know what is your view of how to proceed in the event that hip (femur is anteverted)
Would it be contrary to this article? Should I Avoid Traditional Gluteus and Hip Rotator Stretches?
Thank you!
And congratulations for your excellent education work
Thanks a lot for this article
I’ve had a hip impingement (on both side) 4 years ago during a low bar squat, during months I couldn’t do squats because of the pain, discouraged I infortunately stopped exercising. I’m now back, and I believe that unsolved hip problem provoked knee pain (and IT band pain), I’ve done a lot of clamshells, band walks etc with no results until I found this article, the band mobilizations didn’t do anything for me (no sensation at all, maybe because when I squat now I don’t have any hip pain, just knee pain) but that pigeon stretch is life changing, for the first time I see some improvement !
Thanks for your work
Hi, with hip impingement – what would you say the issue is if the discomfort is more on the inner section of the groin, and exacerbated when i externally rotate at the hip and try to do a hip stretch?
Thanks for the information doc. I started lifting about 2 years ago and realized that no matter how Many times I stretched my hip I could not get low enough to perform a full squat. I recently received an x-ray and was diagnosed with a hip impingement and multiple people told me that because of my anatomy I will never be able to squat. I also have little to no dorsiflexion which is something I also need to work on. even with plates under my heels its still difficult for me to lower into a squat position. I also realize that my feet have always been externally rotated but did not realize that I could have retroversion in my hip. I constantly do pigeon stretches but have never seen the first two that you showed so I will be adding that to my routine. ever since I started lifting this has been one thing that has been constantly bugging me. Its frustrating but won’t give up. if there’s any more advice you could give me on this topic I would be happy to hear it.
Dr. Horschig Thank you! This fixed my hip! It became almost painful to walk, after doing the posterior hip mobilization a few times it was almost gone, this felt like magic!
Can i have hip impingement while i am doing sumo deadlift, but i used to do it year ago with a huge more weight than i am tryin these days and back in the days there was no pain, no uncomfy feelin just felt great natural movement and now i suffer with a serious pain in my hip when i am pressin the bar of the floor. Yes i have same technique that i did last year. I am about to do some hip exercises streches releasing the triggered point and stuff like that and take a step back little bit and hope i can return and even do heavier weights. Yea the question is, is it possible to get a hip impingement this way, like literally maybe from one bad movement. When the whole movement pattern was clearly without any issue in the past. Thanks guys appreciate it
So glad I found this article. I find that my squat is pain free until I start to add weight or start getting fatigued. Would this likely also be a muscle recruitment issue of my glutes as well as my impingement? Do you have any further recommendations? I’ve currently been working on my anterior pelvic tilt issue with floor exercises that “smash” my lower back to the floor, and glute activation exercises using banded clam shells and glute bridges. I will definitely be adding the heavy lateral band movements as well as hip airplanes. It may be that I have information paralysis at this point, I don’t know what I should do as rehab, and what I should do before/while working out?
I can only say that the post is quite helpful; I have read a number of articles and followed the tips given in the driving directions.
Enjoy some time off to goof off and play. Because I have strong opinions regarding this topic, I am interested in learning more about it. Could you kindly elaborate on some of the points you made in your blog post? We shall in fact advance collectively as a result of it Fun Games.
Thanks for the article! Around 4-5 months ago I started getting groin pain and tightness that extended from my inner thigh up to my hip flexors and lower abdomen. Couldn’t work out anymore. Ruled out inguinal hernia. xray showed mild cam/pincer. After not working out for a long time, I suspected it may be my hip causing issues. Tried a few things and ultimately stumbled across this page. Lo and behold after 1 session, my symptoms lessened! More importantly, my hip flexors didn’t completely tighten up after the workout, they even felt a bit loosened up! So, I’m cautiously optimistic that there’s something here.
My few questions are:
(1) how often should I repeat these exercises? Every day? Every other day?
(2) what would you recommend as progressions… ultimately I’d like to return to full sporting activity but just doing these few exercises won’t suffice alone.
I’m grateful that you saved me from this terrible hip pain. have no idea where it originated. Nothing I tried to do worked.