Elbow injuries are often difficult to diagnose and treat. Many educated clinicians find that elbow injuries can be confusing and the treatment can be somewhat complicated. If you look at the research, elbow pain almost always ranks as one of the top injured joints amongst strength athletes like weightlifters and powerlifters.1 However, despite being so common, you can scour the internet and research journals for days and fail to find a consensus amongst medical and rehab professionals on the best approach to its management and treatment.

So why is it so difficult to understand elbow injuries? Let’s start by discussing the anatomy of the elbow joint first.
Elbow Anatomy
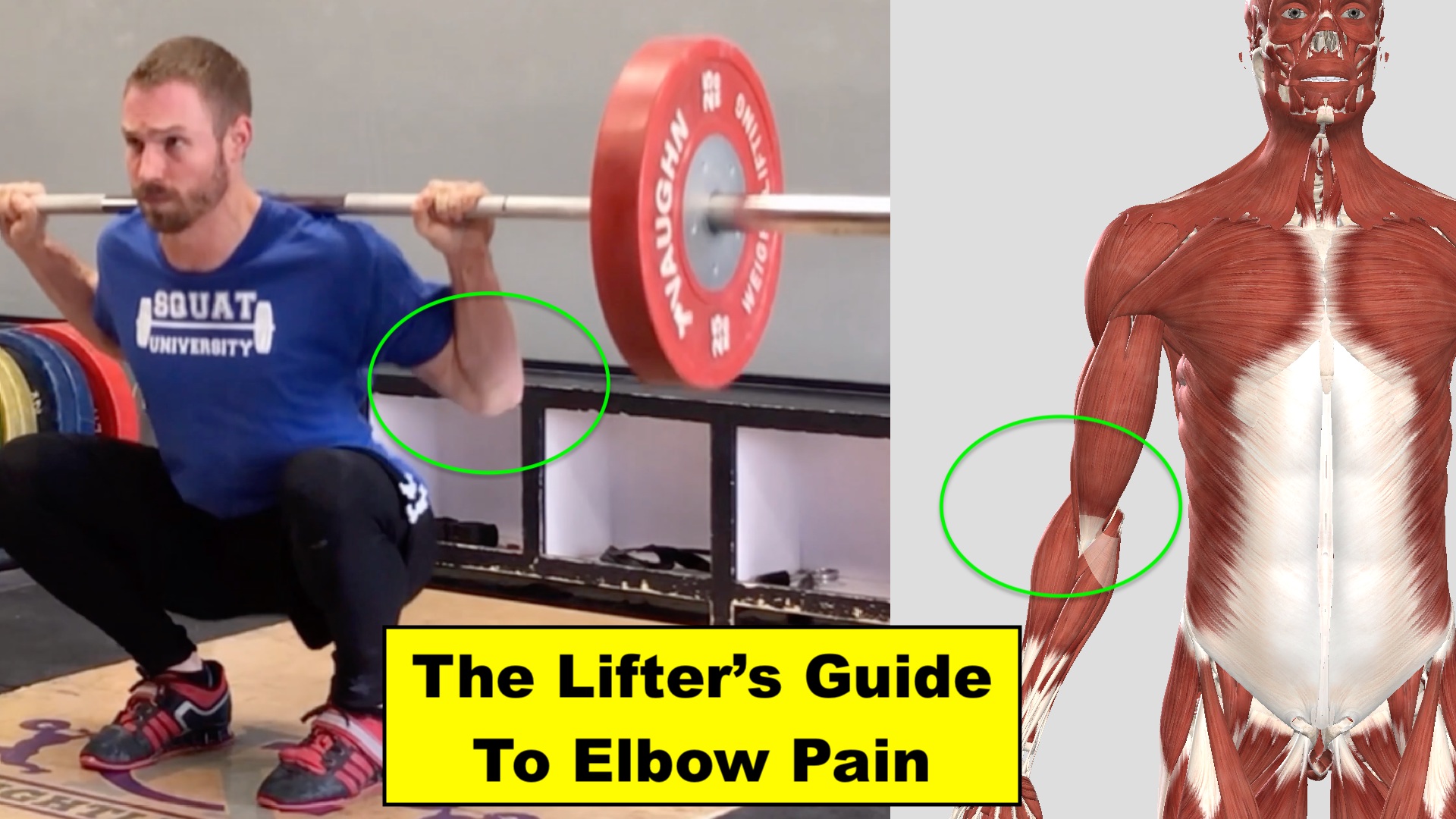
For most clinicians and doctors, most of us are taught that the elbow is a simple “hinge joint,” which opens and closes like metal brackets attaching a door to its frame. To the casual observer this may seem to be true, but there’s much more to the elbow than what meets the eye. Unlike the hinging motion of the knee that occurs between the femur and tibia, the elbow joint contains three bones (the humerus and the radius and ulna of the forearm), which connect to form three small joints.

To make things even more complicated, there are 16 small muscles that cross these joints! Together they work to bend and straighten the elbow as well as rotate the forearm (the motion of pronation and supination).4,7 As you’re starting to see, there’s much more to the elbow than just a simple “hinge joint.”
Screening The Painful Elbow
In order to perform a proper screening of the painful elbow, we need to go through a small checklist:
- Where is the pain located?
- What reproduces the pain in that location?
- Is the pain due to nerve irritation?
The first thing I do when evaluating an athlete with elbow pain is distinguish where exactly their symptoms present. While our rehab plan will never focus solely on the site of pain, differentiating where your symptoms present can help give us insight into the injury mechanism and lead us down the most efficient path for fixing it.
Let’s start with the lateral elbow. The bony nub on the outside portion of your elbow (lateral epicondyle) is the common attachment site for your forearm extensor muscles. Historically pain in this area has been referred to as “tennis elbow” or “lateral epicondylitis.” However, in recent years many have recommended moving away from these two prior terms for a few reasons.

First, inflammation (something the “itis” ending of tendinitis refers to) has not been found in many cases of lateral elbow pain.6 Second, many people develop this injury without ever playing tennis! Instead, pain in this area is now generally referred to as “lateral epicondylalgia.” The pain is often attributed to a tendinopathy (degrading overuse of the tissues similar to a patellar or quad tendon injury).
Injury to this part of the elbow often brings out tenderness when poking just below the lateral epicondyle (where the large extensor tendons of your forearm run and insert). Gripping activities will also often recreate pain (especially when using a palm-down grip or a lift that requires a rotation of the hand from palm-down to palm-up such as a bicep curl).2,3,5

Upon hearing this, many people are confused by how gripping movements can recreate pain at the lateral elbow. Isn’t a gripping exercise performed by the forearm flexor muscles on the opposite side of the arm? The answer is yes.
The muscles on the anterior side of your forearm have the ability to flex the wrist (such as performing a wrist curl) and flex the fingers (make a fist). However, in order to flex the fingers to grip an object like a barbell without any simultaneous wrist movement, something interesting has to happen. Basically the extensor muscles on the backside of the forearm have to kick on in order to stop the wrist from excessively flexing. If the wrist flexors fired and the extensor muscles stayed silent, any gripping activity will be difficult because the wrist will be curled into extreme flexion.7 This means the harder you grip the more load is placed on the common extensor tendon that originates on the lateral elbow.

If we shift to the other side of the elbow, we find another bony nub called the medial epicondyle. This is the common attachment site for a number of your forearm flexor muscles we just talked about. Pain in this area is commonly referred to as “golfers elbow” or “medial epicondylitis, but (just as with the lateral elbow) pain on the inside of the elbow today is now generally referred to as “medial epicondylalgia.”

An overuse injury to this side of the elbow will often create tenderness to tissues surrounding the medial epicondyle that is brought out and made worse when performing resisted wrist flexion (the motion of a heavy wrist curl) or stretching the wrist into extension.7

While the sides of the elbow are often the most common sites of pain for the strength athlete, it is still possible to find injury to the anterior and posterior aspects of the elbow. On the backside of the elbow you’ll find three heads of the triceps converge to form a common tendon that inserts on the olecranon process. On the opposite side lies the attachments of the biceps, brachioradialis and brachialis muscles.
While most cases of elbow pain in strength athletes are due to repetitive overuse of soft tissues (muscles & tendons), symptoms can also be caused by an injury to one of the several nerves that span the arm. Excessive compression or stretch to any of these nerves can create pain in the elbow (often mimicking medial or lateral epicondylalgia), a sensation of “burning,” and radiating numbness/tingling down the length of the forearm and possibly into the hand.7
If you think you are experiencing any of these symptoms, we need to screen your cervical spine to make sure they aren’t stemming from your neck. Start by moving your head as far as possible in every direction. Look up and down, rotate each way and tilt your head side to side as well.
Also look over each shoulder at an angle behind you (creating extension, rotation and a little side bending of your neck) and press down on your head slightly with your opposite side hand. If any of these movements recreate pain in your elbow, I recommend going to see a medical doctor or other rehabilitation specialist for an evaluation. If, however, you did not notice any changes in your symptoms with those neck movements, try these next few screens to determine which nerve may be the source of your pain.
We’ll start with the ulnar nerve that runs on the inside of your elbow. Because of the surrounding anatomy, the ulnar nerve is susceptible to excessive compression, friction and stretching. As the nerve runs down the arm it passes through a small tunnel called the cubital tunnel. When you bend your elbow this tunnel narrows up to 55% of its original size, increasing the incidence of compression and eventual injury.8,11,12

Symptoms of a compression injury to the ulnar nerve at the elbow (called cubital tunnel syndrome) include aching and numbness on the inside of your forearm that may extend all the way to the 4th and 5th fingers or shoot up the arm into the bicep region.7 Movements that pull the elbow into repeated flexion (bench press, pull ups, or receiving the barbell during a clean in the front rack position) or even sleeping on your side with your elbow bent can recreate these symptoms. Over time irritation to this nerve can even progress to limiting your grip strength.
Here’s how to test to see if your medial elbow pain is possibly due to an injury of the ulnar nerve. With your wrist in a straight “neutral” position, bend your elbow as much as you can as if doing a bicep curl and hold this posture for 1 minute. You can also take your thumb of your pain-free arm and push hard into the inside of your elbow (just above the medial epicondyle). This pressure will compress the ulnar nerve that runs underneath. Either of these tests are positive for an injury to the ulnar nerve if they reproduce your symptoms.9,11
Another nerve that can become injured and recreate elbow pain is the radial nerve.25 As this nerve runs down your lateral arm and crosses the elbow joint, it moves through a small passageway between tissues called the radial tunnel. Just like the ulnar nerve on the opposite side of the elbow, the radial nerve has the potential to become compressed and pinched at this area, leading to what is called radial tunnel syndrome. Entrapment of the radial nerve often mimics lateral epicondylagia causing a deep aching or “burning” pain that can extend from the lateral elbow into the hand.25

If you have lateral elbow pain, try this test. Start by taking your opposite hand of the pain free arm and placing it on your shoulder. Pull down slightly in an effort to depress the shoulder and keep it from shrugging upwards during the next portion of the test.

With your symptomatic arm hanging by your side, fully straighten your elbow and turn your hand behind you with palm facing up. Next, make a fist with your fingers clasped over your thumb as if performing a “hookgrip” and curl your wrist slightly (binging your fist towards your forearm). If this doesn’t recreate any pain, slowly raise your arm out to the side. A positive test will reproduce your lateral elbow pain and the intensity of that pain will be modified by either shrugging the shoulder or tilting the head away towards the opposite arm.23,24
As you can now see, there are a number of injuries that can take place at the elbow joint! After going over basic anatomy of the elbow and where injuries commonly present, we can now dive into WHY the pain started in the first place. In order to better understand the cause of your pain, we have to take a step back and look at the whole body.
The Kinetic Chain
Most injuries that occur in the weight room are not dramatic catastrophes (such as a dislocated elbow). They result from wear and tear stresses on the body that accumulate over time. These stresses are influenced by the following factors:
- Mobility
- Stability
- Posture/Technique
Lifting weights places force (called load) on our tissues and joints. When proper loading schemes are carried out with ideal technique and paired with sufficient recovery and rest, the body adapts and grows in its capacity to handle more and more load. Problems arise however when this balanced equation is thrown off due to an issue in any of these factors. When it comes down to the elbow joint, poor lifting mechanics and limitations surrounding mobility and/or stability are often the culprit at fault. For this reason, a thorough evaluation must look beyond the site of symptoms.
I often see frustrated patients who have went through a lot of unsuccessful treatments because the clinician or doctor will treat only the site of pain and they neglect the shoulder girdle or fail to look at movement/actives that cause pain. When it comes to the elbow joint, failed treatment plans usually encompass exercises directed to the forearm muscles and “passive” treatments (ultrasound, tape application, scraping techniques) to the site of pain. While it is not my goal to discredit any of the prior modes of rehab, we are missing the big picture if we never take a step back and look into other possible contributing factors.
Do you remember the childhood song, “the knee bone connects to the thigh bone, the thigh bone connects to the hip bone…” and so on? This seemingly innocent melody is actually something many medical and rehab professionals could learn from.
There’s a saying, “A chain is only as strong as it’s weakest link.” If one link all of a sudden breaks, the whole chain fails. If we look at our body as a linked system or “chain,” it becomes easier to see how a problem at one joint could have direct effect on another elsewhere in the body. The idea of searching out “weak links” in areas other than the site of pain is how we can uncover all of the contributing factors for why an injury occurred in the first place.
Regardless of where your elbow symptoms present, we must start this process by looking at the joints directly below and above the site of pain (at the wrist and shoulder complex).

In order to perform lifts like the snatch, jerk or overhead press, we require a certain amount of wrist mobility in order to create a stable platform for the barbell. Think of the wrist position a gymnast must assume in order to maintain a handstand. The extended wrist position is a vital requirement for creating a sufficient platform to bear weight (whether a gymnast is stabilizing their bodyweight in a handstand or a weightlifter holding a barbell overhead). If an athlete is unable to position their wrist in an efficient weight bearing position while pushing or pulling a barbell or dumbbell, the body is unable to function at an optimal level.

Failure to sufficiently extend the wrist when lifting overhead can lead to excessive forces on smaller structures down the “chain” to make up for this lack of stability.5 Over time this increase in force can lead to an injury at the elbow.
To screen your wrist mobility, pull your hands together and down as far as possible (the prayer pose). Ideally we want to see your wrists move to a 90° “L” position. If you came up short, it could be due to stiff or short muscles in the forearm or limited wrist joint mobility (things we’ll work on fixing shortly!).

Next, we need to search upstream at the shoulder complex. This requires a thorough evaluation of shoulder strength/stability as well as mobility of the thoracic spine, lats and pecs!
There are numerous research studies that have found a connection between weakness in the back and shoulder muscles with the development of elbow pain (especially lateral epicondylagia).15,16,18 Here’s how this cascade of events could unwind. Take for instance someone performing the Olympic lifts of the snatch or clean & jerk. If the athlete lacks proper shoulder stability it will affect their overhead positioning and control of the barbell. This can increase stability requirements to the muscles that surround the elbow joint (in order to keep the bar from falling to the ground), eventually leading to wear and tear overuse injuries.

In this instance, it wouldn’t matter how much effort we place on improving the strength of the overworked elbow musculature, if we never address the lack of stability at the shoulder. It doesn’t always take an expert clinician to remove someone’s initial pain. Eliminate the offending activity (as many doctors will say, “take 2 weeks off barbell training”), prescribe some medication to ease the acute pain, and sprinkle in a few light strengthening and stretching to the surrounding muscles and BAM you’re feeling better! But did a complete fix take place? Or did we just create a short term “window” of temporary relief? I’ll let you be the judge.
In this case, helpful screening tools would be strength tests for shoulder external rotation with the arms by the side and at an elevated position. An inability to maintain the starting position without the hands collapsing in when a force is applied should clue us to take a closer look at the shoulder.
To perform an in-depth screen on the rest of the shoulder complex, check out this blog post.
Once we have uncovered mobility and/or stability deficits at joints above and below the site of pain, we must evaluate lifting technique. This is another area many in the medical community fall short in their injury evaluation process. You can perform all the strength and mobility tests you want, spend thousands on an MRI or CT scan, but if you never watch how someone moves you’ll always fall short in creating a complete analysis.
Let’s go back to the barbell squat example and talk about how it could create pain in the medial elbow. While the slightly extended wrist is optimal in creating a sufficient platform to stabilize the barbell when overhead, using a fully extended wrist to grasp the bar (especially in movements that require a full grip on the barbell) can be problematic. Take for instance the athlete performing a back squat who positions their elbows directly underneath the barbell. Because their elbows are held so low, their only option is to grab the bar with a very extended wrist.

When your wrist is fully extended backwards like this, it places a stretch on the forearm flexor muscles. In this lengthened position, the flexor muscles are unable to exert as much force (compared to a “neutral” straight wrist alignment), meaning grip strength is automatically reduced.27
Trying to maintain a strong grip on the bar with the wrist fully extended increases risk of over working these muscles. Fatigue combined with repetitive training can lead to a chain of events that culminates with wear and tear of the tendons and the potential for developing of medial elbow pain.7 One of the first steps in the rehab process therefore would be to correct the wrist alignment with some simple technique cues to align it in more of a neutral position, which will then take pressure off the medial elbow.

We must also factor in fatigue and how it effects movement quality during certain lifts. Take for example the powerlifter who is performing a high volume day of bench training. If you’ve ever pushed yourself through a difficult workout you know very well that fatigue during repetitive activity can produce changes in movement patterns. While your first set of lifts may look pristine, eventually fatigue sets in and the quality of your reps start to slowly degrade.
Subtle alterations in mechanics when lifting can have profound effects in how your body controls and produces force. For example, research has shown that performing a bench press to the point of significant fatigue leads to a change in technique, decreased strength in the surrounding muscles and increased forces on the elbow joint.19 Over time, substitutions in the way we move and subtle decreases in stability due to loss of strength makes the body vulnerable to overuse injuries.7
For this reason, if you are continuing to lift while you work to fix your elbow pain, it would be wise to manipulate your programming to allow for adequate rest/recovery time and minimize the frequency of repetitive loading so that you can focus on reinforcing proper technique and movement quality.
Fixing Elbow Pain
As you have come to find out by now, there are many different classifications of elbow pain. On top of that, when we bring into account the potential “weak links” above and below the site of pain, we find there are a number of different scenarios for why pain could develop at the elbow. For this reason, there is not going to be a “one size fits all” approach to rehabbing an injury to this joint. We must craft together an individualized plan in order to address your specific elbow pain.
The Global Approach
If you did a thorough job during the prior screening process, you should now have a fairly detailed list of “weak links.” This will help guide your comprehensive approach to fixing the injury (this is called taking a “global” approach as opposed to a “local” approach that only addresses the site of symptoms). Once you have your list completed, scroll back through the prior blog posts on my site to find articles that will help you address each individual factor you’ve uncovered.
One of my favorite exercises that encompasses mobility, stability and movement coordination at the shoulder complex is the paused pull up. Start by hanging from a pull up bar with a shoulder width grip. Completely relax your upper body, letting your shoulder blades pull out to the side of your back as far as possible. For someone with stiffness in their lat muscles, this will bring out a gentle stretch up through your lateral arm pit (where the muscle runs and attaches to the humerus arm bone).
After you have held this stretch for 5-10 seconds, engage these your back muscles by moving the shoulder blades together and down. If you did this correctly the elbows will remain locked into extension (only the shoulder blades move will move as they pull together and down slightly). After holding this position for another 5 seconds, finish the full pull up. If performing the pull up portion of this movement recreates your elbow pain, only perform the shoulder blade stretch and activation movement at this time. Perform 2-3 sets of 5 repetitions.
Using this specific sequence not only addresses lat flexibility but also teaches your body how to properly coordinate movement of the upper body by first setting the shoulder blades into a stable position. Much like the concrete foundation that creates the stability for a house to stand, proper positioning and function of the shoulder blade is vital to the performance and long term health of the elbow joint.
I also like to use the ½ kneeling dumbbell or kettle bell press to windmill. While in a kneeling position, hold a weight by your shoulder in a “racked” position. You can hold your opposite arm out to the side for balance or place it on your torso to give you some feedback for potential rib flaring during the pressing motion.
After you press the weight above your head, hold for a second and feel for the muscles on the posterior shoulder contracting to stabilize the joint. Your shoulder blade should be positioned in a stacked alignment with your arm, elbow and wrist without excessive shrugging by your upper trap muscles.
Next, tip your torso over laterally towards the ground while you keep your hand pointed directly towards the sky. This will mimic the “top-down” sequence of a Turkish kettle bell get-up. As you hold this bottom position, pause and feel for your shoulder blade pulling in towards your spine and the surrounding muscles working hard to stabilize the arm. Finally rotate back up to the start position (making sure to limit excessive shrugging of the shoulder blade) before lowering the weight back to the front rack position. Perform 2-3 sets of 3-5 repetitions.
The concept of improving scapular and shoulder joint stability through exercises like this which target the muscles of the shoulder girdle (trapezius, rhomboids, rotator cuff and posterior deltoid for example) have been shown in research to be a fundamental component to eliminating many symptoms of elbow pain.17
The Local Approach
While I cannot understate how important it is to take a global approach to addressing elbow pain, there are a number of “local” exercises and rehab techniques that can be an extremely helpful addition to a comprehensive treatment plan. These will include forearm strengthening, banded joint mobilizations (specifically with lateral elbow pain), soft tissue mobilizations and nerve gliding.
Isolated Strengthening
Many cases of medial and lateral elbow pain respond well to forearm strengthening during the rehab process.7,24,30,31 It then comes down to choosing the most efficient method of strengthening to fit your injury.
As I discussed earlier, recent research has classified lateral elbow pain a tendinopathy. Isometric exercises (muscle contraction without joint movement) have been shown to be very effective in treating these kind of injuries in the lower body (such as the use of the Spanish Squat for patellar tendinopathy).28 While there is still more research needed at this time in terms of the effectiveness of isometrics in upper body tendon injuries, I have personally found them to be very helpful in many cases with lateral elbow pain.29
For this reason, if you have very inflamed symptoms at the lateral elbow, try isometric holds and see if it can be helpful at modifying your pain. Position your arm over the edge of a table (or across your thigh) and hold a light dumbbell in slight wrist extension for 30-45 seconds for 4-5 reps. If this exercise is right for your body, these should be completely pain free by the 2nd or third repetition and only cause fatigue in the extensor muscles of the forearm. If the exercise is too easy with the weight you’re performing it with, increase the weight until the hold is difficult to perform for the full 45 seconds but can still be performed pain free.

While isometrics can be helpful for many to decrease pain levels, we must eventually move to more traditional strength exercises with movement. Wrist curls (into extension for lateral elbow pain and flexion for medial elbow pain) are the simplest to start with. Perform 10-15 repetitions (with a 3 second concentric raise and 3 second eccentric lower) at a weight you can tolerate for 3-4 sets without increasing pain.24 Tendon injuries often have a delayed response to loading so make sure the difficulty of the forearm strengthening isn’t leading to more pain the following day as well! As strength and pain tolerance improves, increase the weight you are using.

Isolated strength work can also be progressed to more functional movements with carries. The amount of load placed on the wrist extensor muscles during either a single arm “suitcase” or double arm “farmer” carry (due to the neutral wrist position) will be more easily tolerated during the early rehab process for those dealing with lateral elbow pain than the overhand pronated position needed for a front loaded barbell lift like a deadlift.

If you are dealing with lateral elbow pain, eventually we must return to strengthening the wrist extensors in the overhead grip position. An exercise I first saw performed by elite powerlifter Blaine Sumner for this purpose is a rack hold. Start with a barbell positioned around hip height in a squat rack. Grip the barbell with one hand in the very middle. Brace your core and tense all of the muscles from your shoulder down to your hand, then lift the barbell a few inches from the rack. Hold the barbell for 10 seconds before setting it back down. This exercise should be loaded to the point where the 10th rep of 10 seconds if very fatiguing but does not bring out any prior symptoms of pain.
Banded Joint Mobilization with Movement
For some people, their elbow pain can be modified with a joint mobilization exercise. A technique called “mobilization with movement” (MVM) developed by physiotherapist Brian Mulligan, is thought to help correct for a positional fault (problem in alignment and/or movement) of the elbow joint .20,21Essentially, we are attempting to get the joint to move better.
This technique can be especially helpful for those who have a reproduction of lateral elbow pain with gripping activity (making a fist and/or grabbing an object and rotating the hand over and back).
To perform the mobilization, place a thick band (between 2-4 inches in width) across the forearm just below the crease of your elbow. Position yourself on your back with your arm by your side (palm down) so that the band is pulling laterally at a 90° angle away from your body.
With constant tension from the band attempting to pull the arm to the side (creating a lateral joint glide of the elbow joint), perform 10-20 repetitions of clinching and relaxing your fist. You can also hold a small dumbbell in your hand and rotate it band and forth. Make sure to keep your entire arm (other than your hand) flat on the ground. If this exercise is right for your injury and is performed correctly with enough tension from the band, the symptoms of pain with gripping or movements of the hand while holding an object should now be instantly pain-free or greatly reduced during and directly after finishing.21,22,24 If you did not find any significant relief in pain from this mobilization, don’t waste your time performing it as it is likely not right for you.
Soft Tissue Mobilization
For those dealing with almost any type of elbow pain, soft tissue mobilization can be a helpful addition to the treatment process.32 Two useful tools for this process are a small ball (lacrosse or tennis ball) and barbell.
For those dealing with medial or lateral elbow pain, slowly work a small ball between the top of a table and your forearm. Roll it around and seek out spots of tissue that feel tender. Once you’ve arrived at that area, pause for a few seconds before then pumping your wrist up and down for a minute or so. This is an “active release” technique that can help improve tissue and joint mobility.
For those who lacked wrist extension, try re-testing your wrist mobility after the soft tissue mobilization. You may find some short term increases in wrist range of motion following the lacrosse ball self-myofascial release.
For those dealing with symptoms in the posterior elbow or lower triceps, place a barbell in a rack and throw your arm over the top (this specific mobilization is one I first saw from physical therapist Dr. Kelly Starret of MobiltyWOD.com). Pull down on your arm as you slowly glide your triceps up and down the barbell. Just like the prior exercise with the ball, pause on areas of tenderness before moving your elbow up and down for a minute. For some athletes, they might notice improved symptoms directly after the barbell self-myofasical release.
Nerve Related Pain
If you found the prior nerve testing to reproduce your pain, a helpful technique to decrease your symptoms is a nerve glide. Nerve mobilization techniques fall into one of two categories, either aiming to stretch or slide the nerve (relative to the surrounding tissues).10
“Gliding” techniques that stretch the nerve (called nerve tensioning) temporarily increases tension and pressure in the surrounding sheath and may make symptoms worse in some people. On the other hand, “sliders” that move the nerve place significantly less tension on the structure and are therefore less aggressive in mobilizing the nerve in such a way that will not increase symptoms.10 The overall goal of using a nerve mobilization technique is to reduce swelling in and around the nerve, increase blood circulation and to help restore the natural movement capabilities and mobility of the nerve which in turn decreases symptoms.13,14,26
To perform an ulnar nerve “slider,” start with your arm out to the side with your elbow straight and wrist slightly extended (palm up and fingers pointed towards the ground). Next, simultaneously bend your elbow as you pull your arm in front of your body. Keep the wrist in the same extended position this entire movement. Hold this position for a second before slowly moving back to the start position.10
To perform a radial nerve “slider,” you’ll start start in the same testing position as before. Use your opposite side hand to hold your shoulder down. With your arm hanging by your side, fully straighten your elbow and turn your hand behind you with palm facing up. Next, make a fist with your fingers clasped over your thumb as if performing a “hookgrip” and curl your wrist slightly (bringing your fist towards your forearm). Next, raise your arm to the side while you follow your hand with your eyes. Only move to the point where you feel slight tension in your elbow and then return back to the start position.
Make sure you only do a few at a time, as overstressing the nerve (even with a less aggravating “slider” technique) can potentially increase your symptoms. Make sure to also limit any excessive stretching of the wrist flexor muscles, as doing so may irritate the nerve and also intensify symptoms. If these mobilizations help decrease your symptoms, I recommend performing these every few hours throughout your day.
Final Thoughts
As you have now come to learn there is no “one-size-fits-all” approach to fixing elbow pain. However, a thorough screening process (like the one outlined here) can help you develop a program tailored to fit your individual body, allowing you to be that much more efficient in addressing your symptoms.
Unfortunately, there is no quick fix or solution. Treatment will almost always take more time than you would like, but have patience. Nothing complicated was ever solved quickly and as you have learned, the elbow is a much more complicated joint than many realize.
If at any time during this process you experience symptoms that limits your ability to fully straighten your elbow, feelings of the elbow getting “stuck” during movement, a painful popping or clicking sensation, or if you have neck neck pain, I highly recommend seeing a medical doctor or other rehabilitation professional.
Until next time,

With

References
- Aasa U, Svartholm I, Andersson F, Berglund L. Injuries among weightlifters and powerlifters: a systemtic review. Br J Sports Med. 2017;51:211-220
- Bissert LM, Vicenzino B. Physiotherapy managemtn of lateral epicondylalgia. J Physiother. 2015;61:174-181
- Dimitrios, S. Lateral elbow tendinopathy: evidence of physiotherapy management. World J Orthop. 2016;7(8):463-466
- Stroyan M, Wilk KE. The functional anatomy of the elbow complex. JOSPT. 1993;17(6):279-288
- Kaczmarek CM. Lateral elbow tendinosis: implications for a weight training population. Strength and Conditioning Journal. 2008;30(2):35-40
- Waugh, E. Lateral epicondylalgia or epicondylitis: what’s in a name. J Orthop Sports Phys Ther. 2005; 35:200-202
- Hall, CM & Brody LT.Therapeutic exercise: moving toward function (2nd). Lippincott Williams & Wilkins, Philadelphia, 2005.
- Safran MR. El bow injuries in athletes: a review. Clin Orthop. 1995;310:257-277
- Novak CB, Lee GW, Mackinnon SE, Lay L. Proactive testing for cubital tunnel syndrome. J Hand Surg Am. 1994;19(5):817-20.
- Coppieters MW, Bulter DS. Do ‘sliders’ slide and ‘tensioners’ tension? An analysis of neurodynamic techniques and considerations regarding their application. Man Ther. 2008;13(3):213-21
- Novak CB, Lee GW, Mackinnon SE, Lay L. Provocative testing for cubital tunnel syndrome. J Hand Surg Am. 1994; 19:817-20
- Macnicol MF. Extraneural pressures affecting the ulnar nerve at the elbow. Hand. 1982;14:5-11
- Coopieters MW, Bartholomeeusen KE, Stappaerts KH. Incorporating nerve-gliding techniques in the conservative treatment of cubital tunnel syndrome. J Manipulative Physiol Ther. 2004;27(9):560-8
- Oskay D, Meric A, Kirdi N, Firat T, Ayhan C, Leblebicioglu G. Neurodynamic mobilization in conservative treatment of cubital tunnel syndrome: long-term follow-up of 7 cases. J Manipulative Physiol Ther. 2010;33(2):156-63
- Alizadehkhaiyat O, Fisher AC, Kemp GJ, Vishwanathan K, Frostick SP. Upper limb muscle imbalance in tennis elbow: a functional and electromyographic assessment. J Orthop Res. 2007;25:1651-1657
- Lucado AM, Kolber MJ, Cheng MS, Echternach JL, Sr. Upper extremity strength characteristics in female recreational tennis players with and without lateral epicondylalgia. J Orthop Sports Phys Ther. 2012;42:1025-1031
- Bhatt JB, Glaser R, Chavez A, Yung E. Middle and lower trapezius strengthening for the management of lateral epicondylalgia: a case report. J Orthop Sports Phys Ther. 2013;43(11):841-7.
- Day JM ,Bush H, Nitz AJ, Uhl TL. Scapular muscle performance in individuals with lateral epicondylalgia. J Orthop Sports Phys Ther. 2015;45(5):414-24
- Huang YP, Chou YL, Chen FC, Wang RT, et al. Elbow joint fatigue and bench-press training. J Athl Train. 2014;49(3):317-21
- Amro A, Diener I, Bdair WO, Hameda IM, et al. The effects of mulligan mobilisation with movement and taping techniques on pain, grip strength, and function in patients with lateral epicondylitis. Hong Kong Physiotherapy Journal. 2010;28(1):19-23
- Hing W, Bigelow R, Bremner T. Mulligan’s mobilisation with movement: a review of the tenets and prescription of MWMs. NZ Journal of Physiotherapy. 2008;36(3):144-64
- Abbott JH, Patla CE, Jensen RH. The intial effects of an elbow mobilization with movement technique on grip strength in subjects with lateral epicondylalgia. Man Ther. 2001;6(3):163-9
- Coombes BK, Bisset L, Vicenzino B. Bilateral cervical dysfunction in patients with unilateral lateral epicondylalgia without concomitant cervical or upper limb symptoms: a cross-sectional case-control study. J Manipulative Physiol Ther. 2014;37:79-86
- Coombes BK, Bisset L, Vicenzino B. Management of lateral elbow tendinopathy: one size does not fit all. J Orthop Sports Phys Ther. 2015;45(11):938-49.
- Ekstrom RA, Holden K. Examination of and intervention for a patient with chronic lateral elbow pain with signs of nerve entrapment. Phys Ther. 2002;82(11):1077-86
- Arumugam V, Selvam S, MacDermid JC. Radial nerve mobilization reduces lateral elbow pain and provides short-term relief in computer users. Open Orthop J. 2014;8:368-71
- Parvatikar VB, Mukkannavar PB. Comparative study of grip strength in different positions of shoulder and elbow with wrist in neutral and extension positions. Journal of Exercise Science & Physiotherapy. 2009;5(2):67-75
- Rio E, Purdam C, Girdwood M, Cook J. Isometric exercise to reduce pain in patellar tendinopathy in-season; is it effective “on the road?” Clin J Sport Med. 2017;0(0):1-5
- Park JY, Park HK, Choi JH, Moon ES, Kim BS, Kim WS, et al. Prospective evaluation of the effectiveness of a home-based program of isometric strengthening exercises: 12-month follow-up. Clin Orthop Surg. 2010;2(3):173-8
- Raman J, MacDermid JC, Grewal R. Effectiveness of different methods of resistance exercises in lateral epidondylosis – a systematic review. J Hand Ther. 2012;25(1):5-25
- Tyler TF, Nicholas SJ, Schmitt BM, et al. Clinical outcomes of the addition of eccentrics for rehabilitation of previously failed treatments for golfers elbow. Int J Sports Phys Ther. 2004;9(3):365-370
- Starrett K & Cordoza G. Becoming a supple leopard: the ultimate guide to resolving pain, preventing injury, and optimizing athletic performance. Second edition, updated and expanded. Las Vegas: Victory Belt Publishing Inc. 2015. Print
** Special thanks to 3d4Medical and their app Complete Anatomy for the visual of the body in todays post.
Thanks Aaron, this is very helpful.
I have medial pain, usually exacerbated during and after bench press. I’ve tried the first screening test but no pain. There was no pain with the second test either, however if I hold a small ball during the second test while squeezing, the pain appears.
Any suggestions on treating the pain? I’m pretty sure I don’t lack any forearm strength.
Thanks,
Miki.
[…] The Lifter’s Guide To Elbow Pain […]
Interesting stuff to learn about. After reading about strong acids at https://studyhippo.com/6-strong-acids-and-6-strong-bases-flash-cards/ this is a great addition. Thanks for posting!
thanks, when i do the radial nerve test i get a lot of ensations, tingeling etc but no pain, does that matter?
Most detailed article I found so far about elbow pain. Thanks!!!
Hi I liked your article it was very thorough. Now to my question have you heard of Mark Rippetoes ideas for dealing with golfers elbow? He suggests a method called pin firing through chin ups for creating a massive inflammation that causes the tendon to heal faster.
[…] Epicondylalgia, more commonly known as Tennis Elbow, is a common issue where there is irritation of the soft tissue on the outside of the elbow. […]
The elbow joint is a unique connection of three bones and is a complex combined joint that includes three simple joints. Injuries to the elbow joint are particularly common for soldiers in the performance of standards. I read more about the military at https://samplius.com/free-essay-examples/military/. Thank you for your article as a way to keep your readers safe from injury.
Hi, I really appreciate the detail of this article! One think I got lost on was you started talking about anterior and posterior pain:
“While the sides of the elbow are often the most common sites of pain for the strength athlete, it is still possible to find injury to the anterior and posterior aspects of the elbow.”
Immediately after, you transitioned to discussing nerve pain and there was nothing about dealing with anterior and posterior pain. I’m dealing with posterior pain, between elbow and tricep. Seems similar to quad tendonopathy, but in the elbow. Are there different approaches to treating that sort of pain?
Thanks!
This is an amazing type of post.
Safe
Squatting is a great way to stay in shape and can be done anywhere, anytime. Plus, it helps tone your legs, butt and core. If you’re looking to add squats to your daily routine you can become very strong and health person at any stage of life.You can also find best color for concentration on this educational website. It is interesting to read some relaxing exercises here which are enough to keep me fresh.
Squatting is a great way to stay in shape and can be done anywhere, anytime. Plus, it helps tone your legs, butt and core. If you’re looking to add squats to your daily routine you can become very strong and health person at any stage of life.You can also find an idea how to choose essay writing service on this educational website. It is interesting to read some relaxing exercises here which are enough to keep me fresh.
Squatting is a great way to stay in shape and can be done anywhere, anytime. Plus, it helps tone your legs, butt and core. If you’re looking to add squats to your daily routine you can become very strong and health person at any stage of life.You can also find an idea https://www.hrmguide.co.uk/jobmarket/results-oriented-resume.htm on this educational website. It is interesting to read some relaxing exercises here which are enough to keep me fresh.
Any suggestions for treating pronator teres tendonopathy? I had acute pain while carrying a heavy oversized box with outstretched arms and relying on my fingertips to the hold box. I’ve been dealing with this for 3 months and have tried rest, cross tissue message, strengthening exercises using a light dumbbell while performing pronation/supination movements.
If you’re reading this, you probably have a serious case of elbow pain. You may have injured it at work or during a workout (or both). Or maybe you got injured while lifting weights in the gym. Either way, you were referred to me to determine what exactly is wrong and how to fix it. The good news is that I’ve been through this myself and know exactly how bad elbow pain can be. This guide will walk you through my experience with elbow pain, so that when you’re done reading you’ll know everything necessary to take care of an injury like mine. Also read this informative blog roomba 670 vs 690.
sell home newtown Bhai
Can you give us any insights on tricep tendonitis as a result of weight lifting? Thanks!
Yeah! Great!!
As a weightlifter, you understand the importance of maintaining proper form and technique to prevent injury. Unfortunately, even with the best of intentions, sometimes things can go wrong. One of the most common injuries among weightlifters is elbow pain, which can be caused by a variety of factors. In this guide, we’ll explore the different causes of elbow pain and provide you with practical tips and techniques for preventing and managing this type of injury. Whether you’re a seasoned lifter or just starting out, this dyson v6 filter replacement guide is designed to help you stay healthy and pain-free so that you can continue to pursue your fitness goals.
The TEDx Silicon Valley event (tedxsv.org) on May 14, 2011 ron gutman ted, brought together world-renowned thinkers like Ron Gutman to delve into social innovation and the intriguing concept of Living by Numbers. With over 800 attendees and 330,000 online viewers from 50 countries, it proved to be a resounding success, fostering thought-provoking discussions and inspiration. Join the conversation in 2012!
You know that always be fit and donate your plasma and earn with CSL Plasma Promo Code.
Magnifia specializes in providing ERP Software services for specific industries, such as manufacturing, retail, healthcare, and professional services.
Elbow pain is a common issue for lifters, but understanding its causes can make a difference in your performance. Incorporating appropriate warm-up routines and using proper lifting techniques can help mitigate this discomfort. Additionally, while you’re resting from lifting, consider playing a fun game like Funny Shooter 2 to keep your spirits up.
In geometry dash meltdown , players must complete levels by timing their jumps and avoiding traps and obstacles.
This is a fantastic breakdown! You’ve absolutely nailed the complexity and frustration surrounding elbow pain for lifters – it’s something many of us unfortunately deal with. It really resonates with the difficulty in finding consolidated, reliable resources you mentioned, especially with the lack of clear consensus out there.
I’ve personally navigated this, and alongside traditional rehab approaches, finding good tools to support the process was key. On that note, I stumbled upon a platform, funnyshooter.net, which has been surprisingly helpful in managing my own journey. It’s pretty comprehensive, and I was genuinely surprised to find something like it that’s not only completely free and globally accessible but also supports multiple languages and runs smoothly. It’s become a useful part of my toolkit for navigating the kind of challenges you described, maybe offering another angle for those looking for supportive resources.
Thanks again for shedding light on such a common yet tricky issue for strength athletes! Great read.
Access movies and TV shows with vidmate.
Elbow pain, huh? It’s like a bad ex, keeps coming back no matter what you do. But hey, if you want to take your mind off it, check out this gem about a steamy Yuri manhwa. Nothing like a good distraction, right? Drunken My Boss
Elbow pain, huh? It’s like a bad ex, keeps coming back no matter what you do. But hey, if you want to take your mind off it, check out this gem about a steamy Yuri manhwa. Nothing like a good distraction, right? Drunken My Boss
Okay, wow. This is actually super helpful. I’ve been battling this weird ache in my elbow for months now, and yeah, the “hinge joint” explanation never felt right. Sixteen muscles?! No wonder it’s a mess. The checklist is a great starting point. I think mine’s lateral, maybe? Now I gotta figure out what reproduces it. Ugh. I feel like I’m back trying to beat flappy bird – repetitive stress injury waiting to happen! Anyway, thanks for breaking it down like this, really appreciate it. Gonna try some of this out… fingers crossed (carefully!).
Dulu susah nak akses maklumat murid, tapi dengan adanya splkpm, semuanya jadi lebih mudah. Cukup dengan satu splkpm login, ibu bapa boleh pantau. Guru pula manfaatkan splg untuk isi aktiviti mengajar setiap hari.
This really resonated with me. I work in **[kitchen remodeling in Tacoma](https://wakitchenremodelingtacoma.com/)**, and I actually injured my elbow while lifting and doing repetitive work on a job. At first, I thought it was just normal soreness, but it kept getting worse. Reading this helped me understand how complex elbow pain really is and how it’s often connected to movement patterns, overuse, and the whole kinetic chain—not just the elbow itself. It’s a great reminder to focus on proper technique, recovery, and rehab, especially for people doing physically demanding work every day.
The flexibility of this crypto-to-card service is unmatched in the US market right now. I can load it up on Sunday and spend it at the mall on Monday. Clicking on https://virtualcards.com.co/ gave me access to a whole new way of managing my portfolio. It’s essentially a bridge that makes your Bitcoin as spendable as the dollar in your wallet.
A colleague from Australia mentioned this platform and I decided to check it out on a whim. Ended up spending a whole evening there. At https://play-io-casino.com/ the game variety is outstanding — everything from video poker to live baccarat is available. The interface is clean fast and works perfectly on mobile too. Honestly one of the best online casino experiences I have had in a long time.